Public Health Ontario Is Not Being Honest about the Myocarditis Risk in Young Males
And the Canadian government is acting even more irresponsibly.
This week Public Health Ontario recommended that males ages 18–24 no longer be vaccinated with Moderna and that Pfizer be used instead.

PHO stated that in males ages 18–24 myocarditis/pericarditis occurs 5.6x as often after vaccination with Moderna compared to vaccination with Pfizer:
1 in 5,000 vs 1 in 28,000.
But the real incidence of myocarditis/pericarditis following either of the mRNA vaccines is considerably greater than PHO made it seem this week, and we can demonstrate this by using more recent data from PHO itself.
And if we combine those results with data from researchers in Israel the numbers might be much higher still.
What this article shows is that if PHO takes their 1 in 5,000 criterion seriously, neither Pfizer nor Moderna should be given to males ages 12–24. Moreover, Moderna might have to be off-limits to females ages 12–24 as well.
While Public Health Ontario now at least says to no longer use Moderna in males ages 18–24, the Canadian government has authorized Moderna for children ages 12–17. This is a shockingly bad idea, as will also become clear below.

Adjusting for updated PHO data
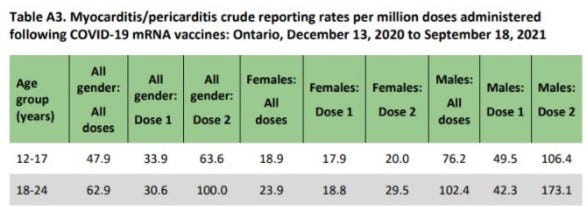
The data PHO used in its recommendation this week are outdated. They are from June 1 till August 7. New data are available from PHO itself and they show a much higher incidence of myocarditis/pericarditis.

For males ages 18–24 this is 42.3+173.1= 215.4 cases for 2 million doses. To simplify the calculation let’s assume everybody had 2 doses (although, in reality, some percentage in that demographic has only had 1 dose so far). This would give an incidence in males ages 18–24 of 215.4 per 1 million people, which is 1 in 4,643.
We don’t know what percentage of vaccines given to males 18–24 were Pfizer and what Moderna. Let’s assume it was 50% each.
If the rate in Moderna is 5.6x that of Pfizer, then we get the following rates for each vaccine:
215.4 divided by (5.6+1) = 32.63
Pfizer: 32.63*1=32.63
Moderna: 32.63*5.6=182.8
Multiply both by 2 to get the per 1 million people rate:
Moderna: 182.76*2=365.6
Or 1 in 2,732
Pfizer: 32.63*2=65.3
Or 1 in 15,314
Those rates are about twice the rates mentioned by Public Health Ontario this week (1 in 5,000 vs 1 in 28,000, respectively).
Adjusting for Israeli data
Israeli researchers, moreover, describe an even higher incidence of 1 in 5,000 in males 16–24 who were given Pfizer (only Pfizer is available in Israel) and they suggest a potential real incidence of 1 in 3,000–6,000 in vaccinated young men.
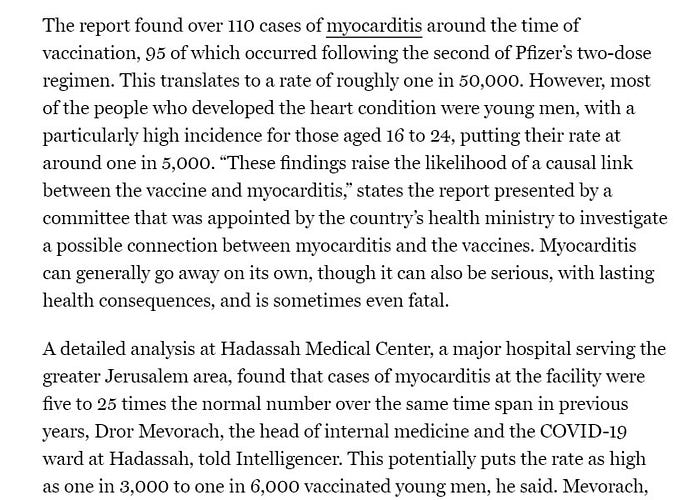
1 in 5,000 is about 3x the rate in the recent data from PHO for Pfizer(1 in 15,314). If we assume that Israeli researchers are correct about the absolute incidence of myocarditis/pericarditis in young males and that Public Health Ontario underreports the absolute incidence but is right about the ratio in which the adverse events occur in Pfizer vs Moderna recipients respectively, this would mean that myocarditis/pericarditis occurs in Moderna recipients at 5.6x the rate of 1 in 5,000, which is 1 in 894.
So if we use the most recent data from Ontario Public Health — data PHO did not use in their recommendation this week — we get an incidence of myocarditis/pericarditis in males ages 18–24:
Pfizer: 1 in 15,314
Moderna: 1 in 2,732
And if we adjust these data to account for the fact that Israeli researcher show a 3.06x higher rate, we get 1 in 893 for Moderna.
Remember, Israel researchers suggested the real incidence may be even higher (1 in 3,000–6,000 vs 1 in 5,000). If we use same assumptions as before but now take the highest Israeli estimate — 1 in 3,000 in Pfizer recipients — we get:
Pfier: 1 in 3,000
Moderna: 1 in 535
Females Ages 18–24
Let’s do the same for females ages 18–24.
The most recent PHO data says 38.3 per 2 million doses, so per 1 million people. If we assume 50% Pfizer and 50% Moderna and if we assume that the rate in Moderna recipients is also 5.6x that of Pfizer recipients we get:
38.3/6.6=5.8
Pfizer: 5.8
Moderna: 5.8*5.6=32.5
Multiply both by 2 to get the per 1 million people rate: 11.6 for Pfizer and 65 for Moderna.
Pfizer: 11.6 per million, or 1 in 86,206
Moderna: 11.6*5.6=65, or 1 in 15,385
Moreover, if we suppose the PHO data underreports actual incidence in females to the same extent as in males (3.06x), we would get:
Pfizer: 1 in 28,172
Moderna: 1 in 5,028
Ages 12–17
Things are even worse for ages 12–17. We know PHO reported incidence per million recipients for boys and girls ages 12–17:
Boys: 49.5+76.2=125.7
Or 1 in 7,955
Girls: 17.9+20=37.9
Or 1 in 26,385
In Ontario ages 12–17 only received Pfizer. But, as mentioned, Canada has approved Moderna for that age group as well. So we can calculate what this would mean if the assumption of a 5.6x higher rate in Moderna were to hold here as well:
Boys: 125.7*5.6=703.9
Or 1 in 1,421
Girls: 37.9*5.6=212.2
Or 1 in 4,713
Moreover, if we assume that there is the same degree of underreporting compared to the Israel data (3.06x), we would get for Moderna:
Boys: 1 in 464
Girls: 1 in 1,540
And if we adjust for the highest Israeli incidence estimate we get:
1 in 278 for boys
1 in 922 for girls ages
Frequency
The frequency of adverse events is expressed using terms such as ‘common, ’rare’, ‘very rare’. Below is the official Adverse Events Following Immunization classification:
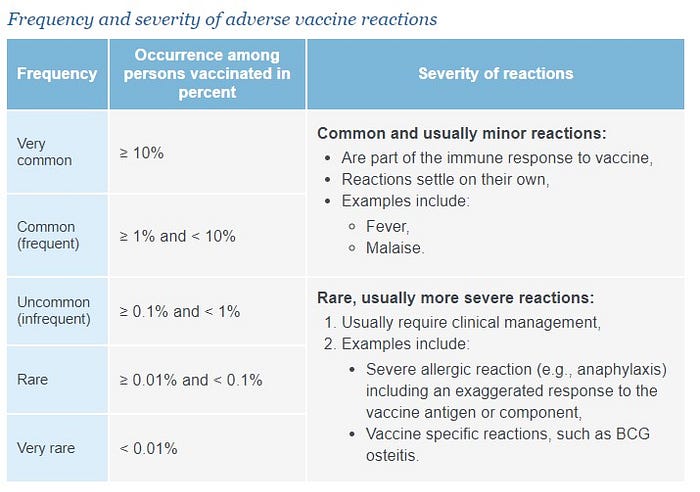
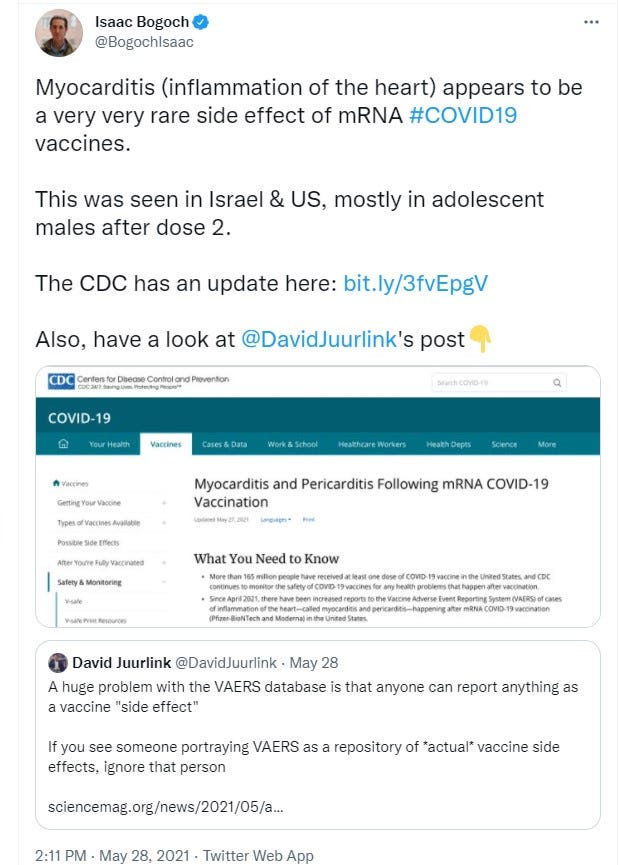
When first reports of myocarditis/pericarditis following immunization appeared several months ago, authorities and doctors emphasized that this adverse event was very rare. Some even called it ‘very, very rare’ which suggests an incidence of less than 1 in 100,000:
This week Public Health Ontario finally acknowledged that in males 18–24 who received Moderna the event was not ‘very rare’ but ‘rare’.
But the calculations in this article suggest this does not go far enough. For Pfizer too myocarditis/pericarditis may not be a very rare but a rare adverse event in males 12–24. Same for females 12–24 who receive Moderna.
Moreover, for males 12–24 who receive Moderna myocarditis/pericarditis may not be a rare adverse event but an uncommon one. For females ages 12–17 the same thing might be true in the highest incidence estimate.
Seriousness
Adverse events are not just ranked in terms of the frequency at which they occur but also their severity. Below is the official classification:
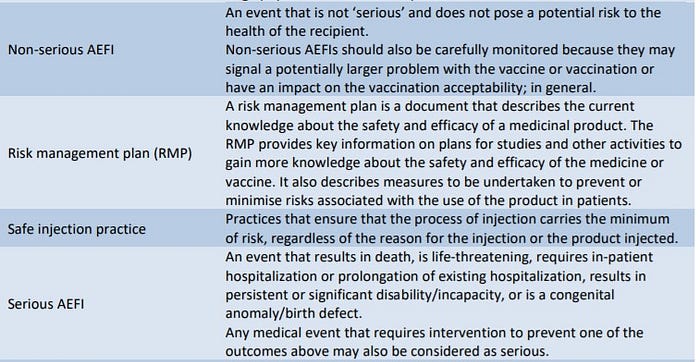
So an adverse event that requires in-patient hospitalization or prolongation of existing hospitalization is a serious adverse event. Public Health Ontario states that 54.9% of the myocarditis/pericarditis patients required hospitalization.

So serious adverse events following immunization with Moderna and for some groups also with Pfizer are not very rare but rare. And if we use the highest incidence estimate for Moderna in males 12–17 and 18–24, serious adverse events may be uncommon instead of rare:
Ages 12–17: 1 in 279
54.9% of which is 1 in 508
Ages 18–24: 1 in 535
54.9% of which is 1 in 975
Recap
Public Health Ontario this week recommended that males ages 18–24 not be given Moderna anymore because of a myocarditis/incidence rate of 1 in 5,000.
Their numbers were based on old PHO data that had much lower numbers than more recent PHO data. Moreover, Israel data suggests that even the most recent PHO data still underestimates actual incidence by a factor 3, or even more if we use their highest estimate.
When we made adjustments on the basis of those assumptions, we get the results summarized in this table:
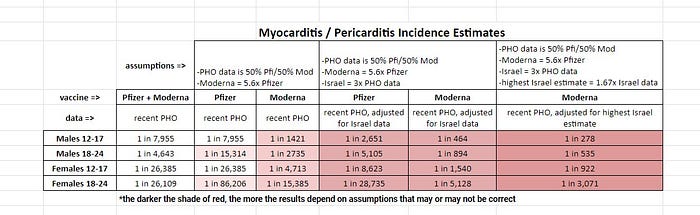
To be sure, the calculations depend on a varying number of assumptions or claims, as described throughout this article and as summarized at the top of the table. Although none of the assumptions seem unreasonable per se, there is no guarantee that all will survive further scrutiny.
Maybe Public Health Ontario’s ratio of a 5.6x higher myocarditis/pericarditis incidence with Moderna than Pfizer is not set in stone, maybe the assumed 50/50 division of Pfizer and Moderna doses among ages 18–24 is different in reality, maybe Israeli researchers overstated or overestimated myocarditis incidence.
And in general, the more assumptions the less reliable the results.
So take the results above with a grain of salt. But don’t dismiss them out of hand. After all, even the calculation that relies on the fewest and the most innocuous assumptions already yields results that show a much higher incidence of myocarditis/pericarditis than admitted by Public Health Ontario in their presentation this week.
Immediate Action
While Public Health Ontario took the right action this week by recommending Moderna no longer be used in males ages 18–24, they were shockingly dishonest in their presentation, and their recommendation does not go far enough. By using their own more recent data I showed that they greatly understated the actual incidence of myocarditis/pericarditis following immunization with Pfizer and with Moderna.
And on the basis of some assumptions as well as data and estimates from Israeli researchers I suggest the real incidence might be much higher still, such that neither Pfizer nor Moderna should be used in males ages 12–24. And that females ages 12–24 should stay away from Moderna as well.
Incredibly, the Canadian government has acted even more irresponsibly than Public Health Ontario, by authorizing Moderna for children ages 12–17.
This is madness.
And it has to stop now.
Update 3: The Alberta Advisory Committee on Immunization now admits to a post dose 2 myocarditis rate in males ages 12-17 of 1 in 2,000. It doesn’t say what the dose 1 rate is but with Pfizer the dose 1 rate in that age group is about half of the dose 2 rate. So put those two together and you get a 1 in 1,333 per person rare (1 in 2,000=50 in 100K. Half of that is 25. So sum of dose 1+2 is 50+25=75 per 100K, is 1 in 1,333)
Update 2: It looks like Public Health Ontario excludes a large number of diagnosed but non-hospitalized cases from its official AEFI report, which would mean that in addition to the now 537 cases in the report, there are thousands more diagnosed cases. See this thread.
update 1: Public Health Ontario published new myocarditis / pericarditis rates today

So the rates new rates are pretty similar to the previous ones: